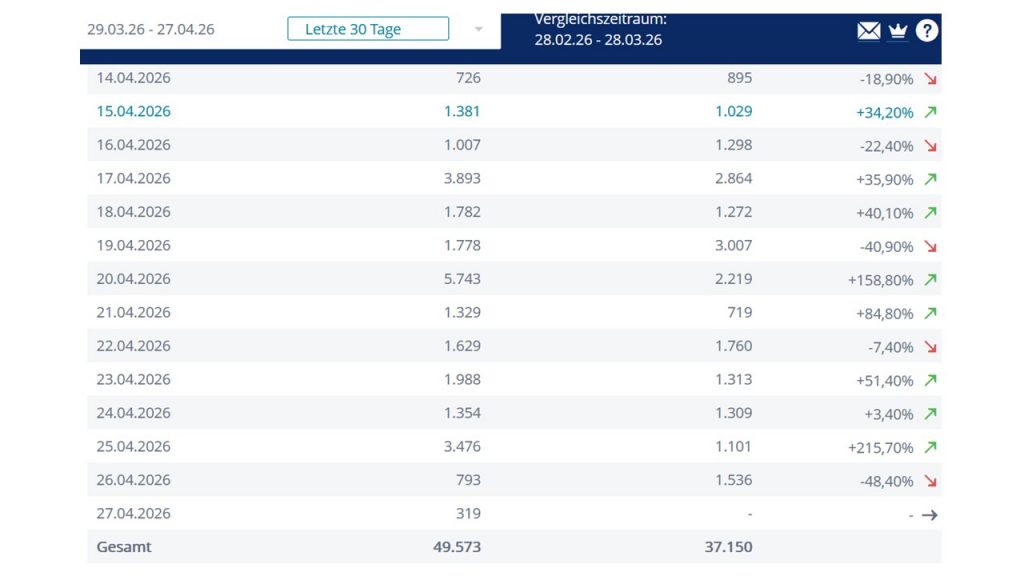
An own webpage “schoemann.org” allows to gain interesting insights into the skills needed for the internet era and the security as well as cost structures for running such a business endeavour. Taking stock of basic web analytics, therefore, should be on the agenda from time to time. Towards the end of April 2026, it is about time to look into some simple statistics again. The host of this webpage offers access to some anonymous statistics (see below). The number of daily or weekly visits of the webpage are suitable to get a basic idea about frequencies of visits. Average daily visits are still below 1000 daily visits, but there are peaks of 3000+ and even 5000+.
Whereas the distribution across weekdays (no peaks on weekends, correlation with bad weather not tested yet ;-)) is rather random compared over months. However, the topics which received most attention are do not seem to be random. In 2026-4 the most attention has been raised with “Abduction of Europa”, followed by a brief entry on “Confessions” a philosophical topic in a broad sense (Stats below 2026-4-27. Next in popularity are 2 entries of my scientific “fail collection” which reflect on take-home-messages from the “Flop exhibition”, quite topical in combination with the 40th commemoration of the Chernobyl nuclear reactor explosion and pervasive contamination across Eastern Europe.
(Image: Page visits between 2026-3-29 to 2026-4-27 compared to month before same year)