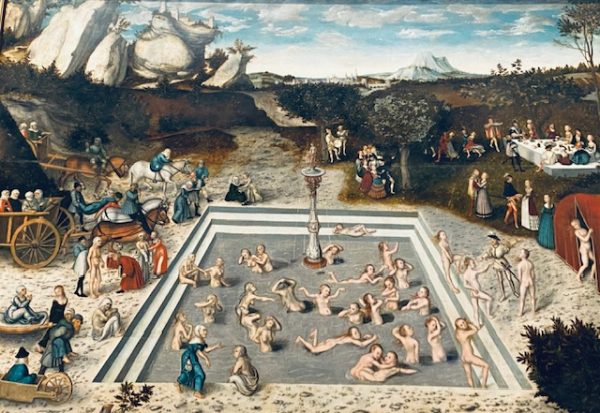
The fountain of youth is such an old dream of humans that we are no longer surprised to witness perpetual reincarnations of the same theme again and again. The painting by Cranach the elder (1646) “Fountain of youth” (image below, Gemäldegalerie Berlin) sets the scene for what has become a billion dollar business nowadays. Whereas the old dream was about rejuvenation and cure from disabling diseases, we have become a bit more moderate in ambition to be happy about a halt to aging. Promises are reiterated and made in building on an army of influencers who push many remedies that lack rigorous scientific tests. Two studies published open access in “The Lancet Healthy Longevity” (Witham, McDonald 2026 and Duremdes Nava et al. 2026) provide evidence that in case of obesity and diabetes there are no easy or quick fixes available yet. Healthy longevity still relies mainly on lifestyle (changes), more exercise and careful nutrition rather than additional medication. Medium and long-term consequences of inactivity and unhealthy diets are to easily disregarded or their value discounted. How much are you willing to pay for an additional year of healthy living at age 30 or 70? Simple economics, but quite a successful business model as well.